Facilitating resource decision making in public organizations drawing upon insights from complexity theory
David Kernick
St. Thomas Health Centre, UK
Abstract
The aim of this paper is to explore how complexity insights can be used to facilitate resource decision making in public systems. The focus is on health care and in particular the UK National Health System. Attempts at rational resource decision making in public systems have identified that there are no explicit frameworks that are acceptable both publicly and politically and that rational decision frameworks are invariably unworkable. This paper explores insights from the UK National Health Service and suggests how complexity insights might be developed to facilitate resource decision making, particularly at grass roots level. The focus moves from the current development of an increasingly methodological competence to creating the conditions for a conversational competence amongst decision makers from which solutions will emerge that may not be optimal but which will satisfy the constraints placed on the system.
Introduction
Against a background of increasing demands on limited health care resources, not everyone can receive the health care from which they can benefit and difficult decisions are inevitable. In market based models individuals make choices based on price, their ability to pay and their individual utility expectations. However, a number of areas of social activity are considered to be more appropriately managed within a public system of resource allocation. Decision making in public systems and in particular the health care sector demonstrates a number of important characteristics:
- A wider range of decision criteria that include appropriateness, efficacy, effectiveness, efficiency, equity and affordability.
- System goals often conflict; for example, efficiency and equity.
- Invariably there is an uncertain relationship between cause and effect.
- There are a number of stakeholders that have different perspectives and specialized knowledge.
- There is a mix of motivations within the system which makes it difficult to align incentives that in some cases can have dysfunctional consequences.
- There are difficulties in engaging the public. Often what the public think, say and do are very different.
- There is a voluminous academic literature which is generally inaccessible and of little practical benefit to those who actually get on and do the work.
In the UK National Health Service (NHS) 80% of resource decisions are taken at a Primary Care Organization level where national policy must be aligned with assessment of local need. Invariably there are conflicting objectives and uncertain causal relationships and rational frameworks have found little application. Can insights from complexity theory facilitate this process?
This paper is constructed in three parts. The first section plots the development of decision making in the National Health Service from hierarchies through markets to the current mixed system that aims to accommodate the best of both approaches. The second section identifies the paradoxes and ambiguities of current decision making frameworks. Finally, some complexity insights for resource decision making are explored.
The development of resource decision-making in the NHS
Historically, decision-making in the UK National Health Service (NHS) has been “a combination of guidelines, exhortation and obfuscation, leaving it largely to the coal faced workers to jiggle a quart of services from a pint pot of resources” (Butler, 1999). Stakeholders were happy to acquiesce to this system where doctors made implicit rationing decisions without challenge, an approach that was flexible and reflected the heterogeneity of patients, doctors and their treatments (Mechanic, 1995) and avoided the disutility of explicit rationing (Coast, 1997).
Over the past decade there has been a call to make decision-making more open. Driven by a more informed consumer and political demands to obtain value for public money, the suggestion is that implicit decision-making may be influenced by professional interests rather than those of patients, is inefficient and incoherent.
To illustrate the evolution of resource decision-making in the NHS a framework proposed by Ouchi, (1980) is developed as shown in Figure 1. This approach sees the mode of operation of health care related to how well the transfer process that relates inputs (resources) to outputs (health) is understood and how accurately outputs can be defined and measured.
The first way: Here the focus is on hierarchy and control.
Decisions are taken within a fixed bureaucratic structure within a framework of predefined rules and regulations. The dominant metaphor of policy analysis and implementation is the machine—each part of the health service with a pre-defined function contributing to the overall purpose with government pulling the levers. In the 1980s a hierarchical managerial approach was consolidated within the NHS that focused on objectives, performance, and accountability.
The second way: This emphasizes the importance of market forces.
In 1989, the UK Thatcher government, outlined a radical agenda, the main features of which were the separation of purchaser from provider function and the development of GP fund-holding within a quasi-market for health (Department of Health, 1989). However, this highly politicized atmosphere split professional allegiances, bewildered the public and caused considerable managerial conflict. In fact, the implementation of managed competition required more rules and regulations than the system that preceded it and overall, despite some changes in culture, measurable changes were small (Le Grand, et al., 1998).
The third way: This approach seeks to integrate cooperation and competition in an attempt to get the best of both worlds.
By the end of the 1990s a political consensus was to develop that acknowledged that the essential features of the market reforms were worth keeping. The new approach to NHS organization was known as the ‘third way’ in health care reform. The theoretical framework had been developed in the mid 1990s by Giddins, (1994) who argued that rigid hierarchical state structures were increasingly incapable of fulfilling the diverse needs of citizenry, and markets alone would not provide economic success or acceptable social outcomes.
The third way advocated a mixed economy that promoted a synergy between public and private sectors, utilizing the dynamics of markets but with the public interest in mind. This pragmatic approach to public policy reform was reflected in the government White Paper: “The New NHS—Modern, Dependable” (Department of Health, 1997). The aim was to retain the elements of the purchaser-provider split but emphasize a more collaborative approach with longer term arrangements. The third way demanded some difficult balancing acts. For example, between central direction or local autonomy, or the use of sanctions or incentives, to direct behavior.
Resource decision making within the context of the third way: The gap between rhetoric and reality
This current search for a mid-path has resulted in a cocktail of organizations and directives issued under the framework of a ‘modernization agenda’. One interpretation is that by making use of a variety of instruments ministers will increase their chances of getting something right!
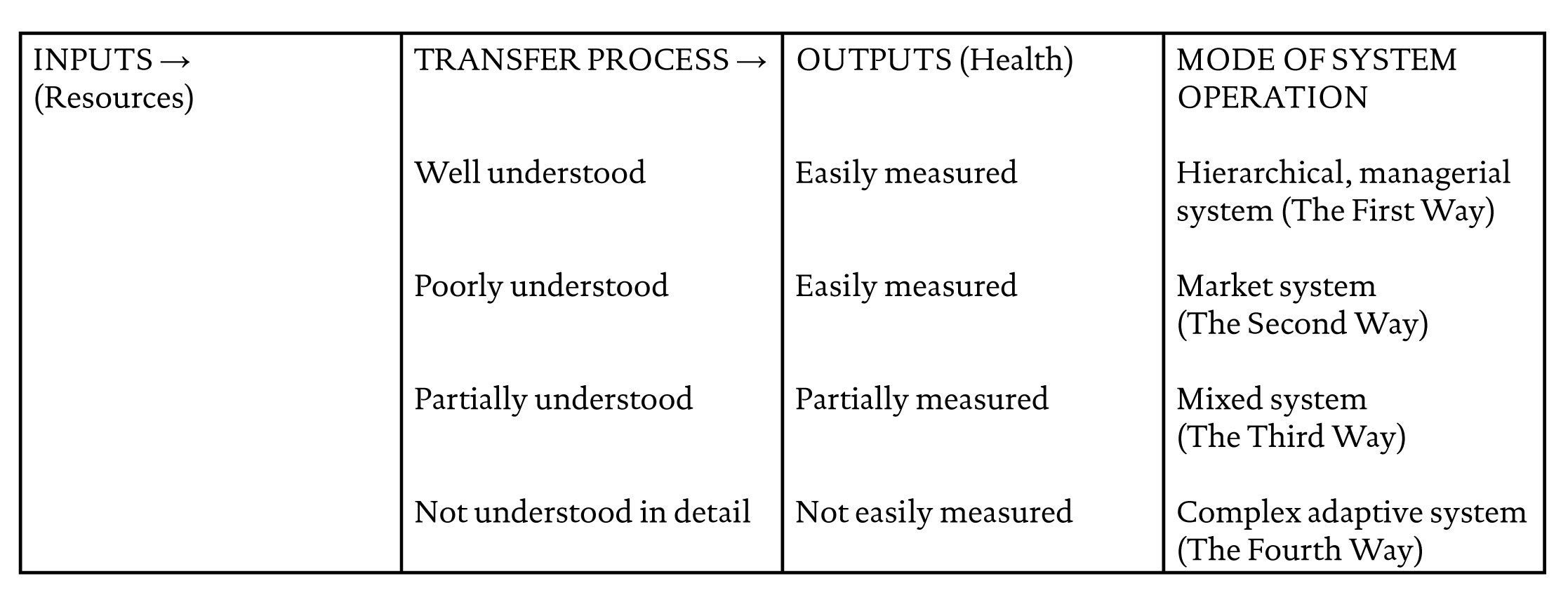
Figure 1 Four models of health systems depending on how well the transfer process that relates inputs (resources) to outputs (health) is understood and how well outputs can be defined
Although a new form of market was introduced under the guise of general practice commissioning, clinical discretion was to be reigned-in within a scientific-bureaucratic framework (Harrison, et al., 2002). National guidelines on clinical interventions were introduced supported by performance management to assess the extent to which health care organizations achieved defined objectives. The National Institute for Clinical Excellence (NICE) makes evidence based recommendations at a national level that are required to be acted upon by Primary Care Organizations, despite the fact that affordability is not a remit of NICE. This framework sits within rational discourses such as health economics and evidence based health care that views resource decision making within a linear and reductionist model over which there is political and managerial control.
Unfortunately, the reality begs to differ. For example, a study of NHS organizations found that the use of technical solutions to resource allocation dilemmas at a local level face substantial barriers which could not be overcome by methodological refinements or the collection of greater volumes of data. Faced with multiple goals, competing objectives and uncertain cause and effective relationships, relating ends to means was highly problematic. In many cases doing something appeared to be better than doing nothing and became an end in itself (McDonald, 2002).
Other studies have demonstrated how managers and practitioners collude to avoid the dissonance between top-down management frameworks and the realities of the health care environment (NHS Public Accounts Committee, 2003). The illusion is maintained that organizations are orderly and rational while at worse, rationality is bounded. If only enough time and processing power were available, an exact solution could be found to any problem.
In reality, when confronted with the paradoxes and ambiguities of organizational life, health care organizations adopt coping strategies (Marshall, 1999; McDonald, 2002). ‘Street level bureaucrats’ process work by modifying their roles and organizational expectations thereby reducing the gap between available resources, practical limitations and system objectives (Lipsky, 1980). Beneath the gloss, the system does not seem to want to do as it is told.
Figure 2 illustrates a case study that demonstrates the difficulties and consequences of applying a linear, rational decision making framework onto a complex, nonlinear system.
In summary, UK attempts at rational resource allocation have reflected international experience that suggests that the process is inherently complex and that there are no explicit frameworks that are acceptable both publicly and politically (World Health Organization Regional Office for Europe, 1996). For example, the Oregon experience demonstrated that ultimately, the primary influence on health service priority rankings was subjective judgements (United States Congress, Office of Technology Assessment, 1992). Simple solutions such as cost effectiveness are often impossible to implement and priority setting by explicit trade-offs are too simplistic to reflect decision making in action.
Figure 3 summarizes the current state of the rationing agenda. Value judgements, estimates and gut feelings remain the predominant determinates of outcome (Honigsbaum, et al., 1995) in an area hedged with constraints, an infinite variety of intermediate positions, arguments and counter arguments.
Complexity insights for resource decision-making
The incremental nature of decision making has been recognized. For example, Butler, (1999) argues that a sensitive and intelligent kind of muddling through seems to accord with the reality of how resources are allocated at the coal-face. Hunter has argued that decision-making in health care is an iterative process, embracing patient intervention and cost effectiveness variables from which a decision is made (Hunter, 1997). In practice, new decisions are invariably compared with previous ones and their rationales in a ‘case law’ that helps to ensure consistency (Martin, et al., 2001). Light and Hughes (2001) identify how economic transactions are embedded in social relationships and argues that rationing is a socially constructed reality that is shaped by cultural beliefs, social norms and power differentials between stakeholders. Mannion and Small (1999) set resource decision making within a post-modern perspective emphasizing the importance of non-mechanistic, metaphorical language. He warns against the increasing esoteric set of concerns of health economists, a trend epitomized by the continual elevation of the mathematical and suggests that knowledge is necessarily multiple, contingent, malleable and dynamic.
How can complexity insights contribute to a pragmatic framework that recognizes the contingencies of decision making in the real world? Nonlinear insights have been incorporated into techniques such as agent-based modelling, but these approaches are generally unavailable and not applicable for the continuum of resource decisions that represent organizational life at a micro-level.
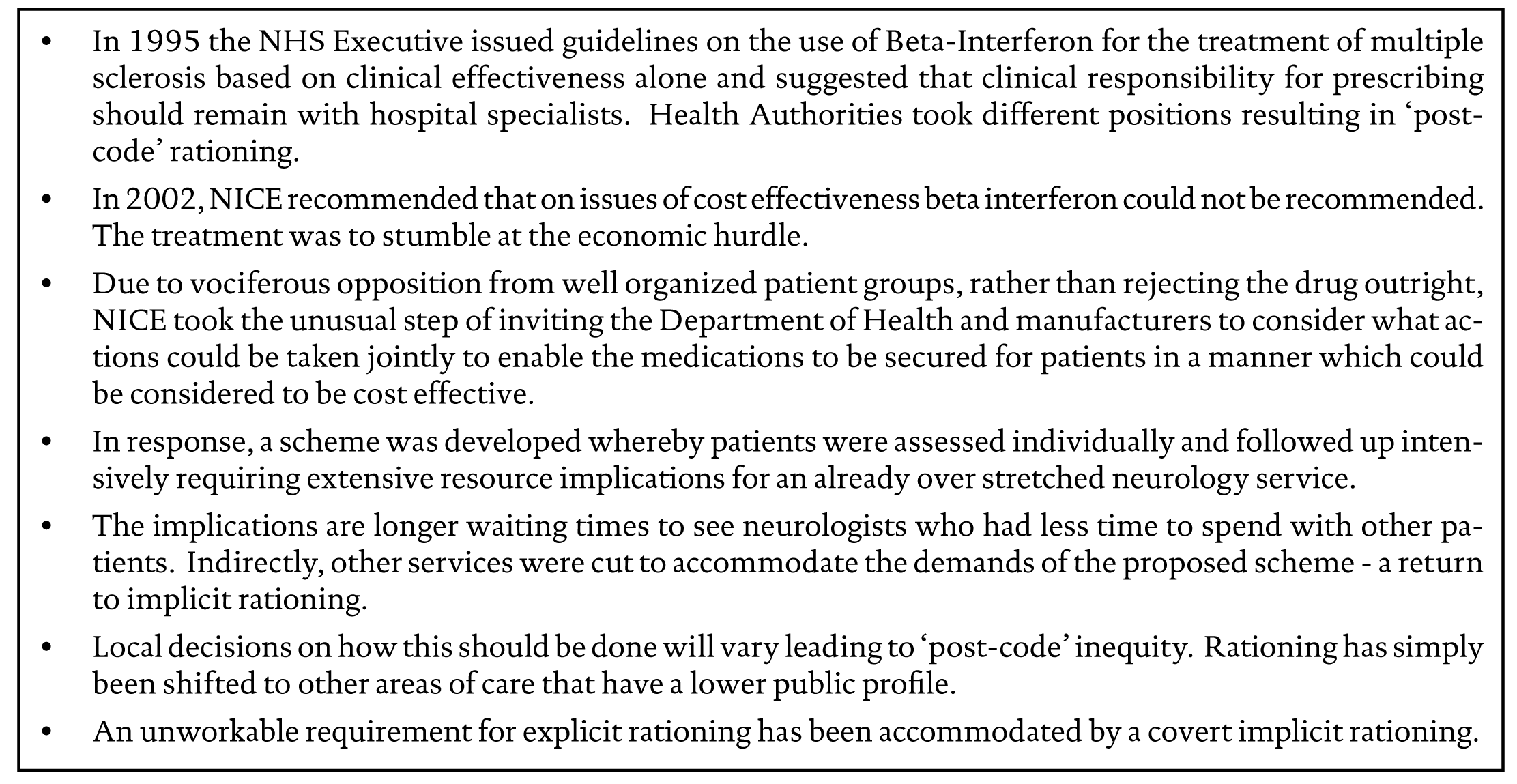
Figure 2 A case study—Beta Interferon and NICE (Kernick, 2002)

Figure 3 Some features of the current rationing debate
Nussabaun, (1995) has suggested that the faculties of mind and the resources of language are best suited to the expression of complex problems. That appropriate emotions are useful in showing us what we might do and also morally valuable in their own right providing the emotion is that of a reflective spectator and not derived from a personal interest in the case. Schön (1982) continues this theme in his analysis of professionals in action. He suggests that competent practitioners usually know more that they can say and exhibit a ‘knowing in practice’. They reveal a capacity for reflection on their intuitive knowledge in the midst of action and in doing so do not solve problems but manage messes.
The essence of any approach would be to recognize that the resources of complexity are best suited to the expression of complex problems through the reiterated and integrated judgement of a collection of stakeholders and experts. Whose interactions organize themselves with reference to themselves into emergent processes from which decisions can emerge as ‘a shared moral sensitivity’. The emphasis is on the interaction between stakeholders rather than their individual properties, interactions that are often inappropriately configured by power relationships. This approach runs counter to the model of technical rationality which sees professional activity as instrumental problem solving made rigorous by the application of scientific theory and technique involving the application of general principles to specific problems.
The key is to develop a conversational competence amongst decision makers rather than the current paradigm of an increasingly methodologically driven one. A reasonableness and sensitivity to the understanding and language that is used, and an ability to escape from one’s own limited vocabulary of knowledge, skills and attitudes. Underpinned by the recursive application of a small number of simple rules or guiding principles, solutions will emerge that may not have been predicted by an examination of the views of each individual stakeholder, that are satisfactory rather than optimal, and provide a platform for the whole process to start again. Figure 4 shows some possible simple rules.

Figure 4 Some ’simple rules’ that could underpin emergent decision-making
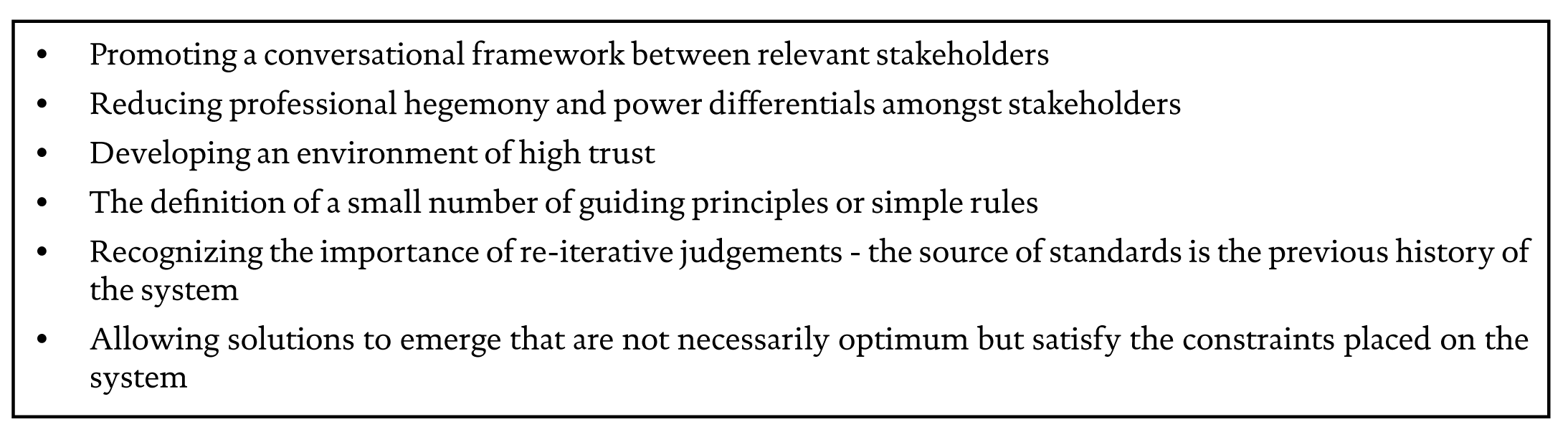
Figure 5 Features of emergent decision-making
Important factors in the success of this framework would be high levels of trust, a mutual understanding of each stakeholder’s perspective and a reduction of power differentials. Here power is used not only in the behavioral sense within a hierarchical framework that implies control of one person over another, but power that resides in the relationships that people have with each other as they try to understand who they are and construct their identities with each other—power as the constraint that excludes some communicative actions and includes others.
In summary, the emphasis is on creating the conditions for emergent solutions by facilitating the interaction of relevant stakeholders. Promoting a conversational framework in an environment of high trust, egalitarian relationships and underpinned by transparent simple rules. Figure 5 summarizes the main features of such an approach.
Conclusion
Perhaps most importantly, complexity theory tells us what we should not be doing. It cautions that we cannot analyze a system by reducing it into its component parts—there are no causal links that promise sophisticated tools for analyzing and predicting system behavior. The first important step is for policy-makers to view the health system as a hierarchy of inter-related systems that interact in a nonlinear fashion. The emphasis moves away from linear rational analysis with the emphasis on prediction and control to an appreciation of the configuration of relationships amongst the health system’s components and an understanding of what creates patterns of order and behavior among them. All elements are seen as co-evolving in a network that is continually transforming itself as an uncertain future emerges with the focus on micro-interaction at a local level.
Rather than spend time on detailed planning and striving to calculate a solution by the continuous addition of rules and measurement, decision-makers should be content with setting minimum specifications, establishing boundaries and letting the system settle into a condition that satisfies the constraints placed on it.
In conclusion, resource decision making is seen as an emergent phenomenon facilitated by the development of a ‘conversational competence’ between stakeholders rather than the increasing pursuit of a methodological one. A move from the ‘science of quantities’ to a complementary ‘science of qualities’. The major challenge is to develop an approach that is both practical and accessible to those who make decisions at grassroots level against a background of a plethora of competing decision frames and counter arguments.
References
Butler, J. (1999). The ethics of healthcare rationing, London, UK: Cassell, ISBN 0304705829.
Coast, J. (1997). “Rationing within the NHS should be explicit: The case against,” British Medical Journal, ISSN 09598138, 314:118-22.
Department of Health (1997). The new NHS: Modern, dependable, London, UK: Her Majesty’s Stationery Office, ISBN 0101380720.
Department of Health (1989). Working for patients, London, UK: Her Majesty’s Stationery Office, Cm 555. Department of Health (2003). Inappropriate adjustments to NHS waiting lists, London, UK: NHS Public Accounts Committee.
Giddins A. (1994). Beyond left and right: The future of radical politics, Cambridge, UK: Cambridge Politics Press, ISBN 0745614396.
Harrison, S., Moran, M. and Wood, B. (2002). “Policy emergence and policy conveyance: The case of ‘scientific -bureaucratic medicine’ in the USA and UK,” British Journal of Politics & International Relations, ISSN 13691481, 4(1): 1-24.
Honigsbaum, F., Richards, J. and Lockett T. (1995) Priority setting and action: Purchasing dilemmas, Oxford, UK: Radcliffe Medical Press, ISBN 1857751000.
Hunter, D. (1997). Desperately seeking solutions, London, UK: Longman, ISBN 0582289238.
Kernick, D. (2002). “Beta interferon, NICE and rationing,” British Journal of General Practice, ISSN 09601643, September: 784-785.
Le Grand, J., Mays, N. and Mullingan, J. (1998). Learning from the NHS internal market: A review of the evidence, London, UK: Kings Fund, ISBN 1857172159.
Light, D. and Hughes, D. (2001). “Rationing: Constructed realities and professional practices,” Sociology of Health and Illness, ISSN 01419889, 23:551-69.
Lipsky, M. (1980). Street level bureaucracy, New York, NY: Russell Sage, ISBN 0871545268.
McDonald, R. (2002) Using health economics in health services: Rationing rationally, Buckingham, UK: Open University Press, ISBN 0335209831.
Mechanic, D. (1995). “Dilemmas in rationing healthcare services: The case for implicit rationing,” British Medical Journal, ISSN 09598138, 310: 1655-9.
Mannion, R. and Small, N. (1999). “Post modern health economics,” Health Care Analysis, ISSN 10653058, 7: 255-272.
Marshall M. (1999). “Improving quality in general practice: qualitative case study of barriers faced by health authorities,” British Medical Journal, ISSN 09598138, 319:164-7.
Martin, D., Pater, J. and Singer, P. (2001) “Priority-setting decisions for new cancer drugs: a qualitative study,” Lancet, ISSN 01406736, 358: 1676-81.
Nussabaun, N. (1995). Poetic justice, Boston, MA: Beacon Press, ISBN 0100998785.
Ouchi, W. (1980). “Markets, bureaucracies and clans,” Administrative Sciences Quarterly, ISSN 00018392, 25: 129-41.
Schön, D. (1982). The reflective practitioner: How professionals think in action, Cambridge, MA: Basic Books, ISBN 046506874.
United States Congress, Office of Technology Assessment (1992). Evaluation of the Oregon medicaid proposal, OTA-H-531, Washington, DC: U.S. Government Printing Office, http://www.wws.princeton.edu/cgi-bin/byteserv.prl/~ota/disk1/1992/9213/9213.PDF.
World Health Organization Regional Office for Europe (1996). European Healthcare Reforms: Analysis and Current Strategies, Copenhagen, www.euro.who.int/observatory/Publications/20020531_1.